United States Health Spending by Race & Ethnicity (2021)
Published August 17, 2021
Video Transcript: It's well established that structural racism and racism impacts healthcare in the United States. Our research team focuses on understanding the $3 trillion of health care spending that occurs each year, and understanding what those resources are used for.
In the study that we just published in the Journal of the American Medical Association, we highlight that a disproportional amount of health care spending is on white (non-Hispanic) populations.
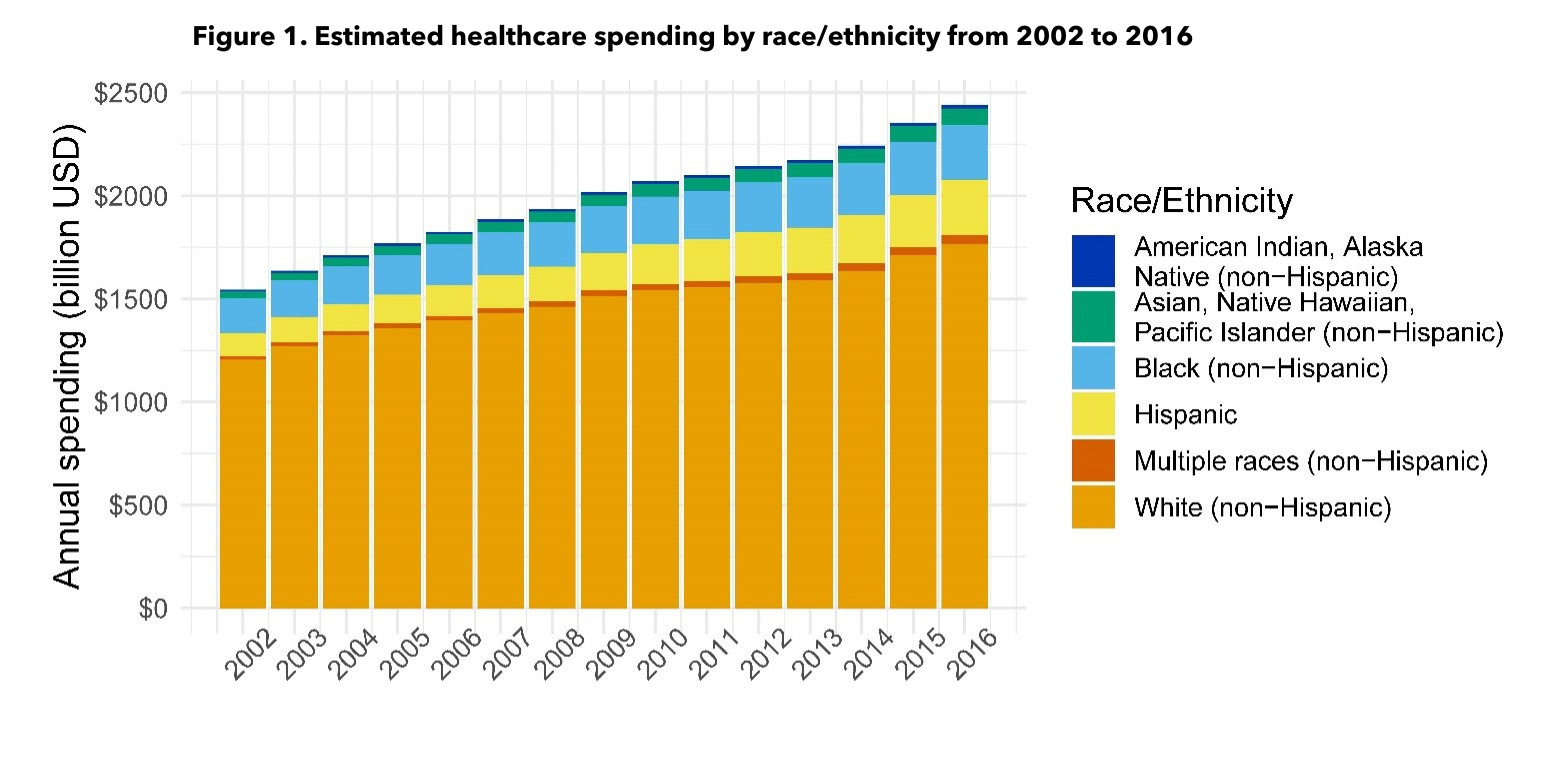
This is health care spending in the United States, disaggregated across these six race and ethnicity groups. The big orange is white (non-Hispanic) individuals. We know that in 2016, all of the spending that we're able to disaggregate, 72-percent of the spending was on white (non-Hispanic)s. That's despite in the United States population that same year, only 61-percent of the the population being white (non-Hispanic). We can see already from this first glance that there's disproportionately more spending on white (non-Hispanic)s.
Despite the variation being less once you've age-standardized in aggregate, the types of care that the different race and ethnicity groups were having spending on really varies dramatically.
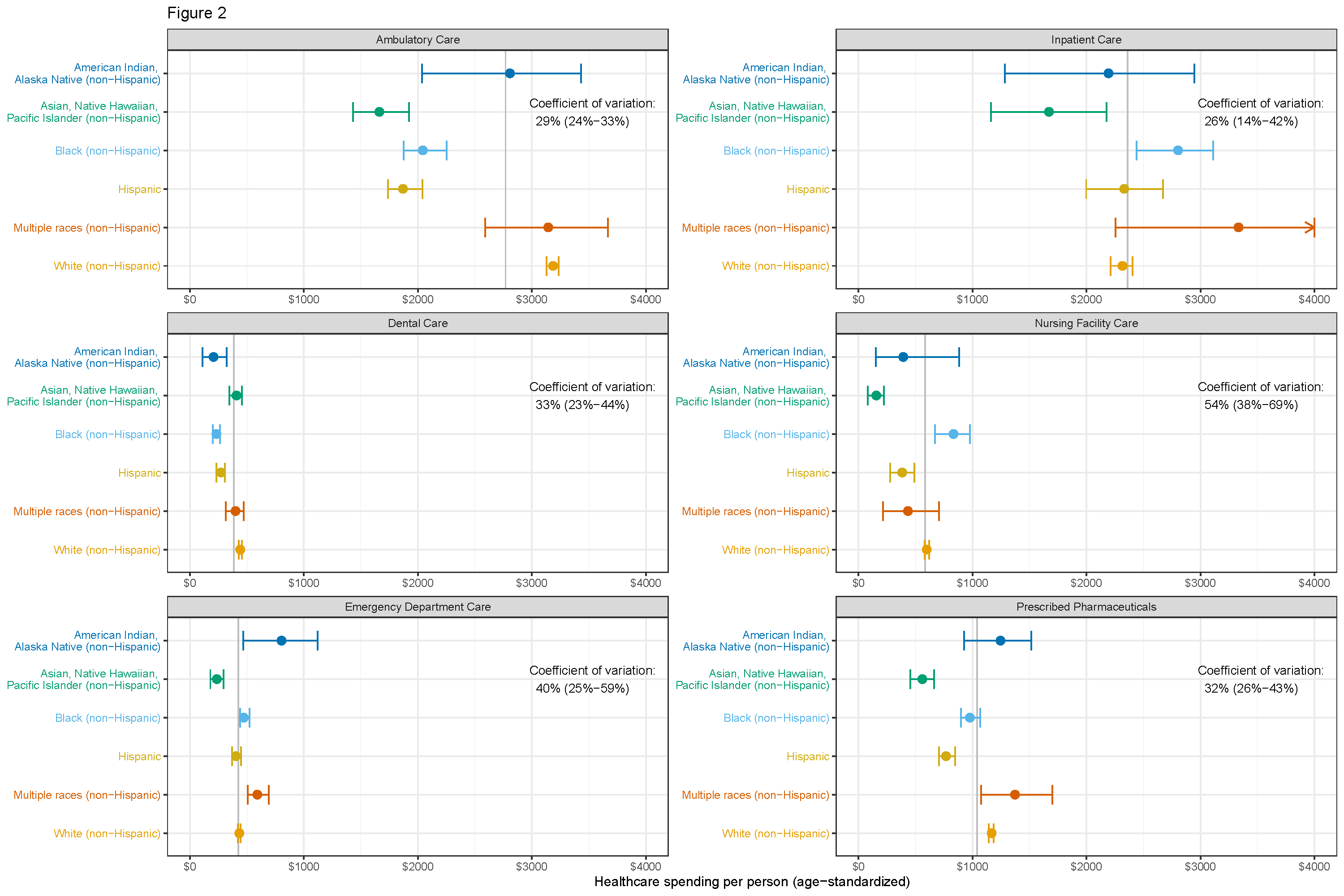
This first slide here looks at ambulatory care, so outpatient care, and dental care. You can see the average amount of spending for people within each one of those race/ethnicity groups for outpatient care and dental care. The gray line is the all population mean. So we can see on the panel on the left if you focus just on ambulatory care, the Asian American, Native Hawaiian, Pacific Islander, Black, and Hispanic groups all spend significantly less on ambulatory care per capita after age-adjusting and the white non-Hispanic population spends way more.
Switch over to emergency department care and inpatient care, you see much more parity in spending. You see Black (non-Hispanic) actually spending more than Hispanic and white non-Hispanic in emergency department care. And in inpatient care, you see more or less of the the same trends.
Lastly, you can look at nursing facility care and prescribed pharmaceuticals. For both of these, we see that the Hispanic population is lower and the Black (non-Hispanic) is a little higher. And in the prescribed pharmaceuticals, white (non-Hispanic) is higher too.
Moving forward, we think that it's especially important to think about the allocation of health care resources. In particular, driving up utilization for key essential services for preventive care and care for Black, Indigenous, and people of color populations in the United States to drive up and improve health equity.