
Prevent COVID-19 deaths by prioritizing interventions for Hispanic, Latino, and Black populations in the US
Published November 24, 2020
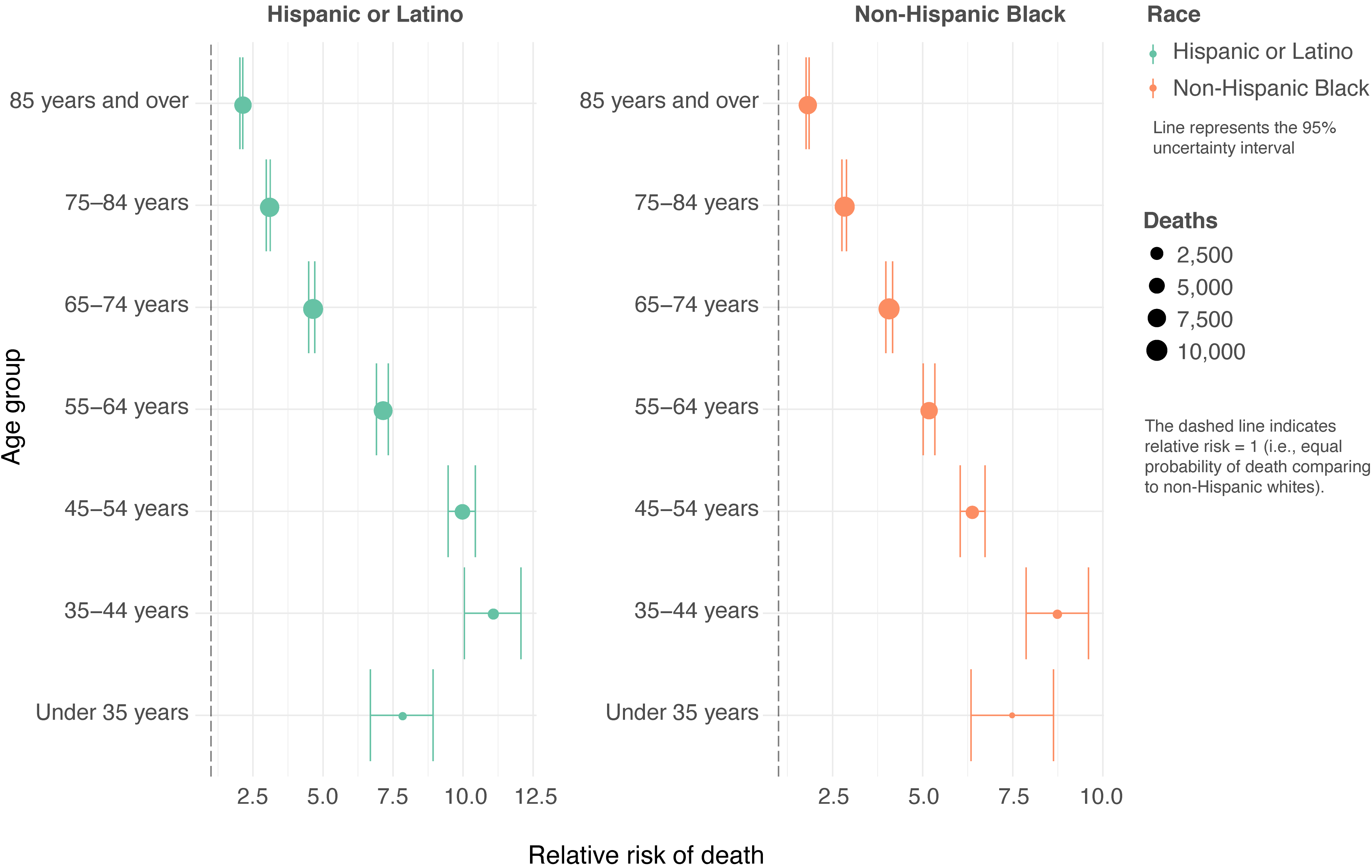
Analysis by IHME comparing the risk of dying from COVID-19 by race and ethnicity confirms that Hispanic or Latino Americans, and non-Hispanic Black Americans are more likely to die from COVID-19 than non-Hispanic whites. The excess risk is also higher among younger age groups, indicating that work exposure is one potential source of this disparity. This highlights an opportunity to save lives by prioritizing lifesaving interventions (such as masks and other PPE) at work and in social interactions. This also suggests that the groups at disproportionately higher risk of mortality should be prioritized as new developments, such as effective vaccines, become available in the coming months. The elevated risk in Hispanic, Latino, and non-Hispanic Black Americans means that their risk of death at age 50 is equal to the risk of death for a 65-year-old non-Hispanic white American.
What are the risks for Hispanic and Latino populations?
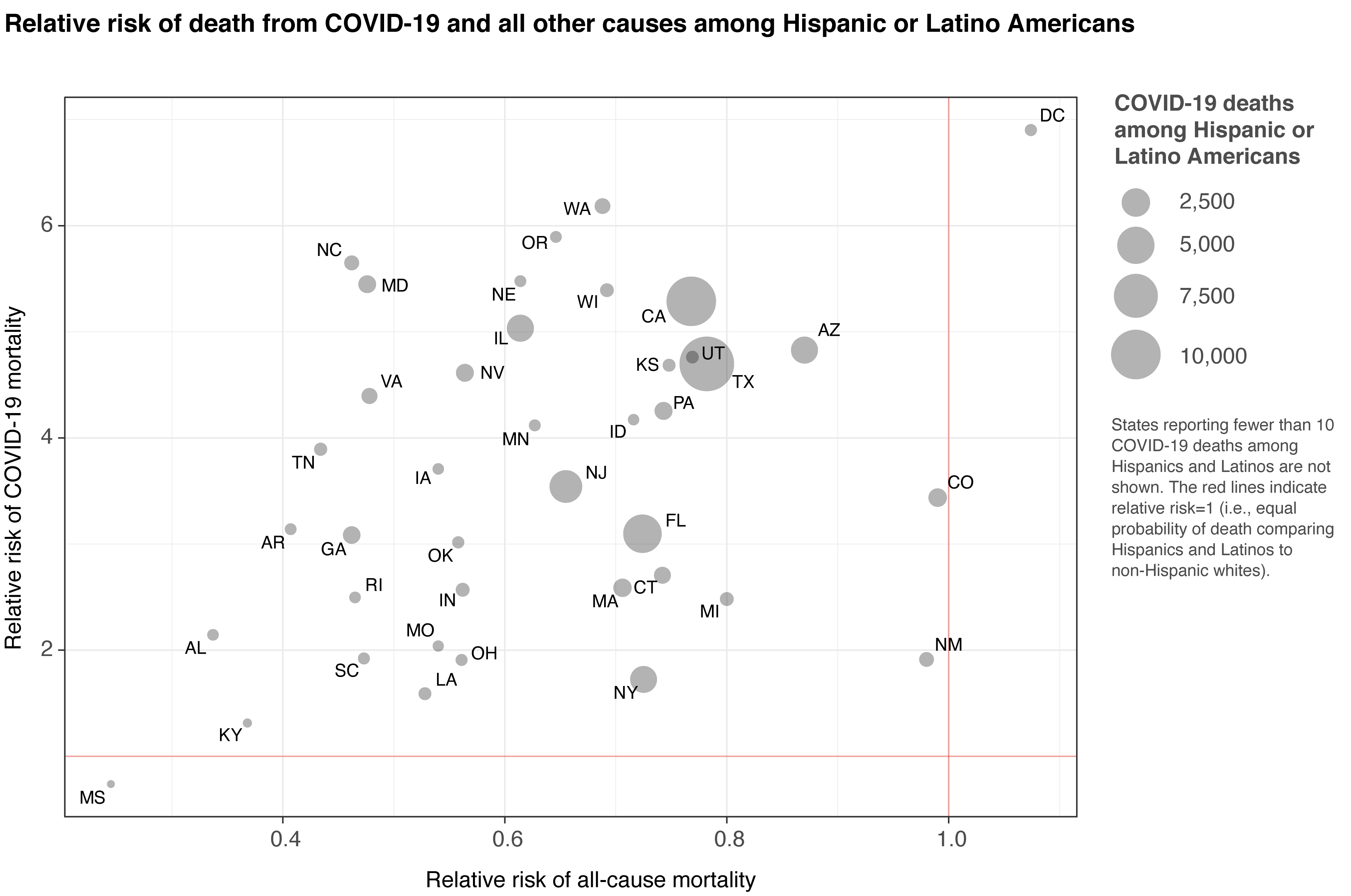
Across the US, COVID-19 mortality is much higher among Hispanic and Latino populations than non-Hispanic whites. The risk of dying from COVID is up to 6.9 times higher for Hispanics in the 40 states that have recorded more than 10 deaths among Hispanics. This underscores the urgency of addressing this disparity. Hispanic populations in the US have generally experienced a lower risk of all-cause mortality compared to non-Hispanic whites, but COVID-19 is hitting much harder.
What are the risks for Black populations?
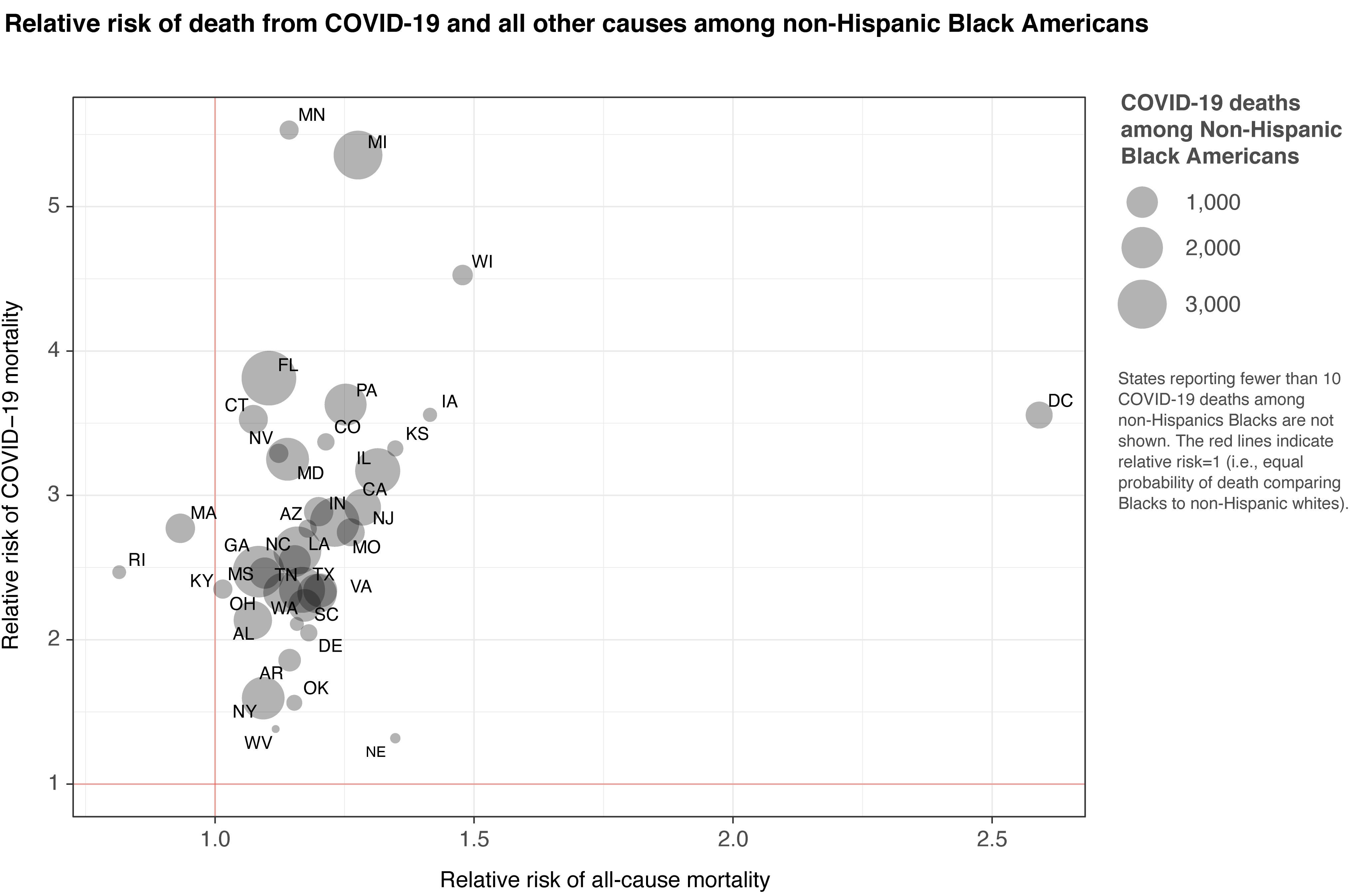
Similarly, COVD-19 mortality is much higher among non-Hispanic Black populations than non-Hispanic whites. For non-Hispanic Black Americans, who were already at higher risk of death from all causes than whites, the risk of dying from COVID is up to 5.5 times higher across the 38 states that have reported more than 10 deaths among the non-Hispanic Black population. In this way, COVID-19 has exacerbated existing disparities and will worsen these disparities in the future unless decisive action is taken.
Where is the problem most acute?
For Hispanic and Latino populations, the disparities are highest in DC and parts of the West and Midwest. Texas and California are two states with both high numbers of deaths and very high disparities for Hispanic and Latino populations. For non-Hispanic Black populations, disparities are highest in parts of the Midwest and in Florida. For both groups, there is large geographic variation in the disparities.

What age groups face the most excess risk?
Working-age Hispanic, Latino, and non-Hispanic Black Americans are more likely to die from COVID-19 than non-Hispanic white Americans in the same age group. These findings suggest that excess risk may be disproportionately affecting individuals who cannot work from home. Racial disparities in who is able to work remotely, versus needing to show up for work in person, should be investigated further as a source of increased COVID-19 exposure.
What factors are contributing to increased risk?
Disparities in health outcomes are generally due to socioeconomic factors, access to medical care, quality of medical care, and preventable risk factors. Our data suggest that the key factor in the increased risk of COVID-19 death among Hispanic, Latino and non-Hispanic Black Americans is increased exposure to the virus, probably because these populations are less likely to be able to work from home. These findings could be used in designing and implementing preventive programs to reduce exposure through protective measures, such as mandating use of masks, gloves, or other PPE at all times, and ensuring adequate PPE supplies for essential workers. Moreover, our findings show the value of preventing infection in the first place in the US. Most important, we need measures enacted now to protect our essential workers, ensuring that adequate food and supplies are available. The goal should be to avoid the need to shut down certain businesses such as meat packing, which we saw in the beginning of the pandemic. While we await a vaccine, we all must adopt the same core strategies that have proven effective to date: wear a mask, maintain social distancing, and wash hands.
What are the data sources and limitations?
IHME has leveraged all available data, but there are some states with small numbers of deaths for Black and Hispanic populations, making it more difficult to analyze trends.
Data on COVID-19 death counts by state, age, race, and Hispanic origin group were downloaded from the National Center for Health Statistics (NCHS) at CDC (last downloaded on November 12, 2020). These data present cumulative deaths since February 1, 2020, that were identified on the decedent’s death certificate as a death due to COVID-19 (ICD-10 code U07.1). The database lists a 1−8-week potential lag time between the date a death occurred and the date the death appears in the dataset due to delays in state reporting of death certificate data to the NCHS. Age is reported by 10-year age groups from 5 to 85, with additional “Under 1,” “1−4 years” and “85 years and above” categories. Race/ethnicity data are reported in the following categories. For the purpose of this analysis, IHME has focused on the two populations with the largest numbers of deaths due to COVID:
- Hispanic or Latino
- Non-Hispanic White
- Non-Hispanic Black
- Non-Hispanic American Indian or Alaska Native (AIAN)
- Non-Hispanic Asian
- Non-Hispanic Native Hawaiian or Other Pacific Islander (NHOPI)
- Non-Hispanic More than one race
Notably, race/ethnicity classification is drawn from the race/ethnicity variable recorded by a funeral director and is not self-reported, leading in some cases to differences between decedents’ self-identified race/ethnicity and the race/ethnicity to which they are classified in this dataset. Due to small numbers, analyses for groups other than Hispanic or Latino, non-Hispanic white, and non-Hispanic Black are not included here. Additionally, states with fewer than 10 deaths in a race/ethnicity category are not shown.