
New study shows US health care dollars disproportionately spent on White Americans
Published August 17, 2021
Analysis from Institute for Health Metrics and Evaluation highlights need for urgent action to eliminate health disparities
SEATTLE — A new analysis of US health care spending reveals stark disparities across racial and ethnic lines, with White Americans benefiting from an outsized share of health care dollars relative to their proportion of the population. The study, conducted by researchers from the Institute for Health Metrics and Evaluation (IHME) at the University of Washington School of Medicine, was published today in the Journal of the American Medical Association. IHME’s analysis shows that the differences in spending are driven by inequities in how Americans utilize health care, with minority patients less likely to receive outpatient services or prescription drugs.
“This study provides a clear picture of who is benefiting from and who is being left behind in our health care system,” said Dr. Joseph L. Dieleman, Associate Professor in the Department of Health Metric Sciences at the University of Washington and lead author of the study. “Measuring disparities in health care spending and use not only helps us understand the magnitude of inequities, but also provides valuable insights for policymakers to address their underlying causes.”
The study reveals that in 2016 non-Hispanic White Americans received health services representing 72% of all health care spending, despite comprising only 61% of the population. On the other hand, Hispanic and Asian Americans received the least spending relative to their proportion of the population: Hispanic patients benefited from 11% of health care spending despite accounting for 18% of the population, while Asian, Native Hawaiian, and Pacific Islander individuals received 3% of spending while making up 6% of the population.
Figure 1. Estimated health care spending by race/ethnicity from 2002 to 2016
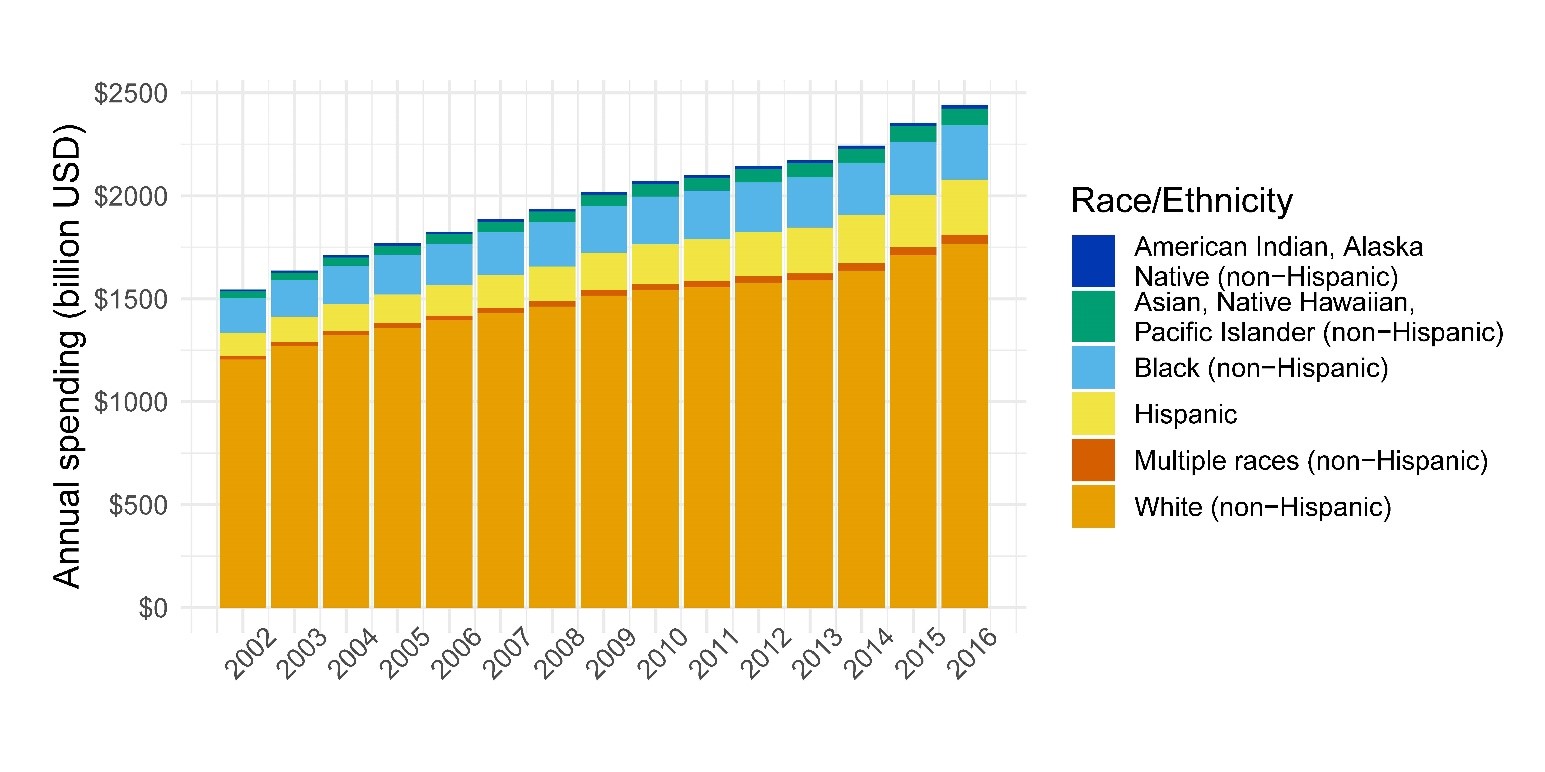
In 2016 non-Hispanic White Americans (denoted by the orange section) received health services representing 72% of all health care spending, despite comprising only 61% of the population.
“Latinos in particular often lack access to high-quality health care and are among the least likely of any racial or ethnic group to visit the doctor when they have a medical issue,” said Amelie G. Ramirez, DrPh, director of the Institute for Health Promotion Research and the Salud America! program at UT Health San Antonio. “As a result, they suffer from poorer health outcomes on a range of measures. This study highlights the urgent need for new investments in Latino health.”
While spending on African Americans was roughly equal to their share of the population – they received 11% of health care spending, while making up 12% of the population – it was skewed significantly toward emergency and inpatient care, suggesting that they do not receive care until they are experiencing advanced illness. Specifically, they received 26% less spending on outpatient care, but 12% more spending on emergency department care.
“COVID-19 has exacerbated health disparities,” said Dr. George Mensah, director of the Center for Translation Research and Implementation Science within the National Heart, Lung, and Blood Institute at the National Institutes of Health (NIH). “This paper adds to existing research that illustrates the need for comprehensive solutions to address underlying barriers patients face in achieving optimal health and benefitting from optimal health care.”
IHME’s analysis shows that differences in health care utilization across racial and ethnic groups explain the majority of spending inequities. White Americans received 15% more spending on outpatient care than average, suggesting they have better access to routine and preventive care. They also receive more spending on dental care and pharmaceuticals than other groups. Non-White Americans, on the other hand, were less likely to visit ambulatory care or receive prescriptions. When they did access care, it was more likely to be in emergency or inpatient settings.
These findings persist when adjusting for differences in disease prevalence across racial and ethnic groups. The study also found that price and intensity of services were not major drivers of spending disparities, with only a few significant differences in the cost of healthcare services for different groups.
This study included data from 7.3 million health system visits, admissions, or prescriptions captured in the Medical Expenditure Panel Survey (2002–2016) and the Medicare Current Beneficiary Survey (2002–2012). These data were combined with insured population estimates from the National Health Interview Survey (2002; 2016) and healthcare spending estimates from the Disease Expenditure project (1996–2016). In 2016, an estimated $2.4 trillion was spent on health care across the six types of care included in this study – outpatient care, dental care, emergency department care, inpatient care, nursing facility care, and prescribed pharmaceuticals.
The IHME study also adjusted for differences in the age structure of each group, something few studies comparing health care spending by race and ethnicity have adequately done. Age is a known driver of spending and adjusting for differences in the age distribution of different groups is necessary for valid comparison. This is also one of the only studies to analyze health care spending by race and ethnicity after implementation of the Affordable Care Act.
About the Institute for Health Metrics and Evaluation
The Institute for Health Metrics and Evaluation (IHME) is an independent global health research organization at the University of Washington School of Medicine that provides rigorous and comparable measurement of the world’s most important health problems and evaluates the strategies used to address them. IHME is committed to transparency and makes this information widely available so that policymakers have the evidence they need to make informed decisions on allocating resources to improve population health.