Search results
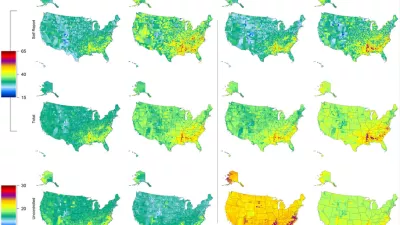
Prevalence, awareness, treatment, and control of hypertension in United States counties, 2001-2009
Hypertension is an important and modifiable risk factor for cardiovascular disease and mortality. We estimate trends in prevalence, awareness, treatment, and control of hypertension in US counties using data from the National Health and Nutrition Examination Survey (NHANES) in five two-year waves from 1999–2008 including 26,349 adults aged 30 years and older and from the Behavioral Risk Factor Surveillance System (BRFSS) from 1997–2009 including 1,283,722 adults aged 30 years and older.

Big data opportunities for global infectious disease surveillance
It is perhaps surprising to state that we have an extremely poor knowledge of the global distribution of the vast majority of infectious diseases. Here we argue that this information gulf has serious implications for global public health surveillance and that too little attention is given to spatial epidemiology in international preparedness planning.

The Global Burden of Disease: Generating Evidence, Guiding Policy
The Global Burden of Disease: Generating Evidence, Guiding Policy provides an overview of the reasons why the Global Burden of Disease (GBD) is an essential tool for evidence-based health policymaking and summarizes the main findings of the Global Burden of Diseases, Injuries, and Risk Factors Study 2010 (GBD 2010). GBD 2010 is the most comprehensive study of its kind, producing comparative metrics for 291 different causes of premature death and disability across 187 countries, 20 age groups, and both sexes for three time periods: 1990, 2005, and 2010. The study also estimated 67 potentially preventable causes of ill health, or risk factors, such as smoking, high blood pressure, and household air pollution.

UK health performance: findings of the Global Burden of Disease Study 2010
The United Kingdom has provided universal health care and public health programming for more than six decades. To guide future policymaking in the UK, it is important to analyze trends in population health over time. Using data from the Global Burden of Diseases, Injuries, and Risk Factors Study 2010 (GBD 2010), researchers examined three critical questions: what are the patterns of health loss in the UK, what are the leading preventable risks that explain some of those patterns, and how do UK outcomes compare to a set of comparable countries in the European Union (EU) and elsewhere in 1990 and 2010.

The Stability of Malaria Elimination
Summary When the Global Malaria Eradication Programme (GMEP) was launched in 1955, all malaria-endemic countries outside of Africa were (or would soon be) eliminating malaria. The GMEP's design was based on a theory of malaria transmission dynamics and control that has become the standard for malaria elimination decisions today. When financial support for the GMEP collapsed in 1969, participating countries were caught at different stages of progress toward elimination. Examining their fate in the decades that followed provides a natural experiment that tests the theory. With a rise in funding and renewed interest in eradication, there is now a need to revisit the lessons learned from the GMEP. We identify changes in the epidemiology of malaria when elimination is reached that could explain its stability and discuss how this calls for a reassessment of strategies for eradication.

Nets, spray, or both? The effectiveness of insecticide-treated nets and indoor residual spraying in reducing malaria morbidity and child mortality in sub-Saharan Africa
These findings suggest that greater reductions in malaria morbidity and health gains for children may be achieved with ITNs and IRS combined beyond the protection offered by IRS or ITNs alone.

Financing Global Health 2012: The End of the Golden Age?
Financing Global Health 2012: The End of the Golden Age? is IHME’s fourth annual report on global health expenditure and includes preliminary estimates for health financing in the most recent years. In this year’s report, IHME built on its past data collection and analysis efforts to monitor the resources made available through development assistance for health (DAH) and government health expenditure (GHE). It confirms what many in the global health community expected: After reaching a historic high in 2010, overall DAH declined slightly in 2011, with some organizations and governments spending more and others spending less.

Global mapping of infectious disease
The primary aim of this review was to evaluate the state of knowledge of the geographical distribution of all infectious diseases of clinical significance to humans.

Incorporating loss to follow-up in estimates of survival among HIV-infected individuals in sub-Saharan Africa enrolled in antiretroviral therapy programs
Measuring the survival of human immunodeficiency virus–infected adult patients enrolled in antiretroviral therapy (ART) programs is complicated by short observation periods and loss to follow-up. We synthesized data from treatment cohorts in sub-Saharan Africa to estimate survival over 5 years after initiation of ART.

Results of the Global Youth Tobacco Survey and implementation of WHO Framework Convention on Tobacco Control in former Soviet Union countries
The prevalence of ever smoking and current smoking, smoking initiation, and exposure to second-hand smoking decreased over time. Overall, willingness to stop smoking, supporting smoking bans, and receiving information about the dangers of smoking increased over time.

Years lived with disability (YLDs) for 1,160 sequelae of 289 diseases and injuries, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010
Individuals, households, and health systems devote enormous resources to curing, preventing, and eliminating non‐fatal, disabling health conditions. Therefore, it is essential that some form of measuring and tracking non‐fatal burdens be available for policy and planning purposes.

Age‐specific and sex‐specific mortality in 187 countries, 1970–2010: a systematic analysis for the Global Burden of Disease Study 2010
The number of deaths in each age and sex group for countries, regions, and the world is a critical starting point for assessing the Global Burden of Disease (GBD). A careful estimation of deaths and mortality rates by age and sex is essential to assess progress, improve health, and extend the lives of people around the world. Information about mortality rates and causes of death at different ages, especially premature mortality, is also an important impetus for public policy action.

Healthy life expectancy for 187 countries, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010
Healthy life expectancy, or HALE, is a measure of average population health summarizing both mortality and non‐fatal outcomes. HALE is used for comparisons of health across countries or for measuring change over time. These comparisons can shed light on key questions about how morbidity worsens or improves as mortality declines.

Common values in assessing health outcomes from disease and injury: disability weights measurement study for the Global Burden of Disease Study 2010
Measurement of the global burden of disease using disability‐adjusted life years (DALYs) requires disability weights that measure health losses for all non‐fatal consequences of disease and injury. There has been vigorous debate over the definition and measurement of these weights. The primary objective was a comprehensive re‐estimation of disability weights through a large‐scale, population‐based, empirical investigation in which judgments about health loss associated with many causes were elicited from the general public in diverse communities. This is a marked improvement over previous efforts, which relied solely upon judgments from a small group of health professionals.

Disability‐adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010
In this paper, results on years lost due to premature mortality (YLLs) and years lived with disability (YLDs) are combined to examine the overall burden of disease across 291 diseases and injuries by country for the period 1990 to 2010.

Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010
The goal of this research was to estimate deaths and years of lives lost (YLLs) by age, sex, and region for 235 causes at two points in time – 1990 and 2010. This information can be used to better inform global efforts to assess whether society is or is not making progress in reducing the burden of premature – and especially avoidable – mortality.

A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010
The goal of this study is to calculate what proportion of deaths or disability‐adjusted life years (DALYs) can be attributed to specific risk factors, holding other independent factors unchanged. Quantification of the disease burden caused by different risks informs prevention by identifying which risks make the greatest contribution to poor health. No complete revision of global burden of disease caused by risk factors has been done since a comparative risk assessment in 2000, and no previous analysis has assessed changes in burden attributable to risk factors over time.

Disentangling the effects of risk factors and clinical care on subnational variation in early neonatal mortality in the United States
Between 1990 and 2010, the U.S ranking in neonatal mortality slipped from 29th to 45th among countries globally. Our objective is to measure the extent to which trends and subnational variation in early neonatal mortality reflect differences in the prevalence of risk factors (gestational age and birth weight) compared to differences in clinical care.

Exploring the relationship between population density and maternal health coverage
This engenders the hypothesis that population density positively affects coverage rates of health services. This hypothesis has been tested indirectly for some services at a local level, but not at a national level.

Does distance matter for institutional delivery in rural India: an instrumental variable approach
This paper estimates the causal effect of distance to health facility on institutional delivery in rural India, taking into account the endogenous placement of the health facility. We find that women living closer to health facilities are more likely to give birth at health facility.

In denial: misperceptions of weight change among adults in the United States
While many Americans reported losing weight between 2008 and 2009, the actual prevalence of obesity in the United States increased over this time period, according to researchers at IHME. Results from the study “In denial: misperceptions of weight change among adults in the United States” show that public health officials should interpret self-reported weight losses with caution.