
New report reveals nearly half of malnutrition-related deaths in those with cleft could be prevented with access to adequate treatment and support
Published October 7, 2022
Globally, for every 1,000 live births, 1.41 babies are born with orofacial clefts and almost 195,000 babies are born with clefts each year. Currently, 4.62 million persons are living with an unrepaired or inadequately repaired cleft, making them susceptible to a number of potentially life-threatening conditions and increasing their risk of malnutrition.
Children younger than 5 years with clefts endure a heavier burden of poor nutrition and risk for malnutrition. Globally, they are 2.15 times more likely to be underweight and at risk for growth failure compared to the general under-5 population. The unique anatomy of the lip and/or palate reduces the ability to create suction during breastfeeding and bottle feeding, impacts muscle coordination needed for swallowing, increases the possibility of food inhalation and aspiration pneumonia, and extends the time required for feeding. Collectively, these challenges result in lower intake of food and diminished health status. Smile Train, an organization that works with local doctors and cleft care providers in over 90 countries globally, has partnered with the Institute for Health Metrics and Evaluation (IHME) to quantify the combined burden of malnutrition and clefts to reduce the prevalence of malnutrition in individuals affected by orofacial cleft abnormalities.
According to Smile Train, there is a widespread lack of global data related to cleft and malnutrition, and the organization was “interested in working with IHME to work through the cleft burden with global malnutrition and mortality data to answer those questions that have never been answered on a global scale.” To quantify the contribution of child growth failure among those with clefts to the global burden of malnutrition, Smile Train merged their existing data with estimates of the direct health consequences of malnutrition from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD). They used underweight as a proxy to generate comparative estimates of the rate of malnutrition from 60 low- and middle-income countries in children younger than 5 years by age, sex, location, and year.
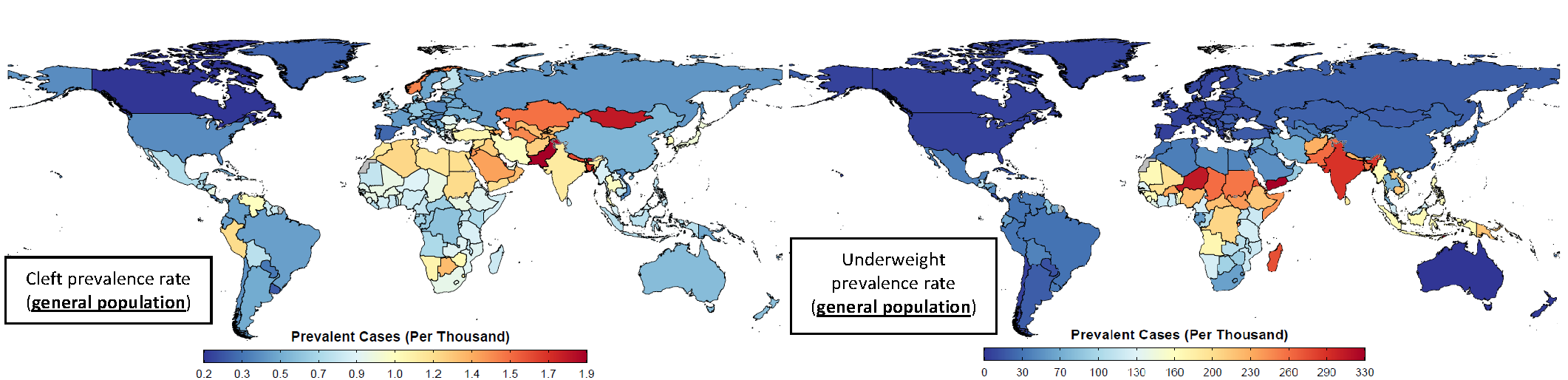
In 2020, nearly 600,000 children younger than 5 years were living with clefts, and of those, 200,000 were underweight. The highest cleft prevalence rates were in countries in North Africa and the Middle East, extending into Central Asia and South Asia. Cleft prevalence rates were lower in sub-Saharan Africa, with about 1 in 1,000 children having a cleft in those countries. However, sub-Saharan Africa (from Sahel to the Horn of Africa) and South Asia had the highest rates of underweight conditions, increasing the vulnerability of those with clefts to malnutrition.
Source: Quantifying the Burden of Malnutrition in Children with Orofacial Clefts: Summary Report
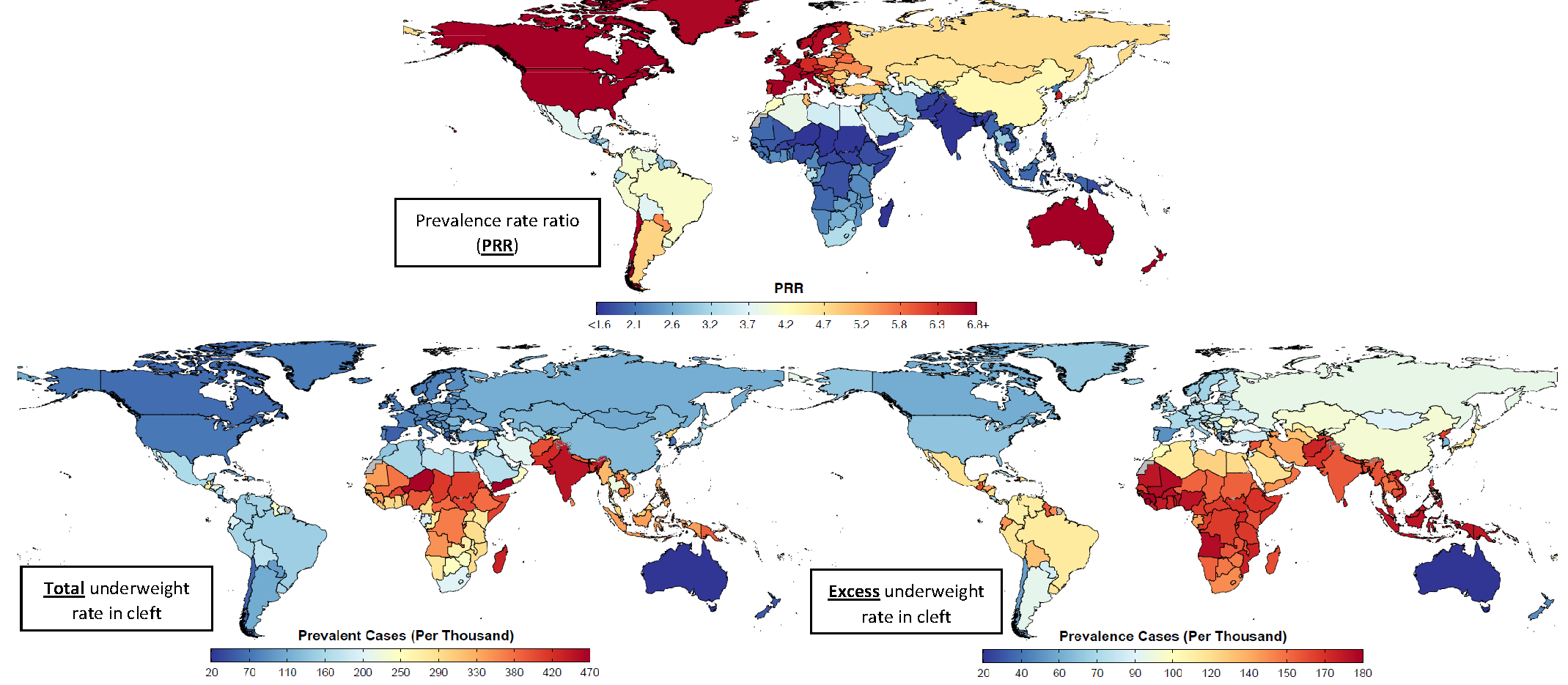
The prevalence rate ratio (PRR) was also used to estimate the comparative risk of malnutrition in those with clefts to the general population. When combining PRR with population-level estimates of cleft anomalies and underweight condition, those in sub-Saharan Africa, South Asia, Oceania, and Southeast Asia had the highest excess rates of underweight. Countries in peri-Sahelian Africa, Somalia, Pakistan, and India had an excess burden when combined with GBD deaths per case of underweight. As indicated by the data, children with orofacial clefts have an increased vulnerability to malnutrition, regardless of the economic, social, cultural, and political context of a country. Between 2000 and 2020, more than 46,000 children with clefts died as a result of malnutrition. Half of malnutrition-related deaths in those with clefts could be prevented with access to adequate treatment and support.
Source: Quantifying the Burden of Malnutrition in Children with Orofacial Clefts: Summary Report
Dr. Nick Kassebaum, a pediatric anesthesiologist and researcher in this collaboration, said that it is important to recognize “how much further [children with cleft] can fall behind and how much more vulnerable they are than the general population, needing extra attention to avert disaster.” Existing interventions and treatments include feeding modifications, specialized equipment and education for parents, psychosocial risk assessments, frequent weight monitoring, and surgical repair, preferably before 3 months of age. While this is an extensive spectrum of interventions, the number of children born with clefts and the size of the under-5 population with clefts experiencing malnutrition have failed to decline significantly over the past 20 years. There remain 1.8 million excess cases of underweight condition in the cleft population, and these cases are concentrated in sub-Saharan Africa and South Asia, warranting additional care in countries with both high cleft prevalence and underweight rates.
Dr. Kassebaum recommends that the interventions needed are two-fold: “1) Support for nutrition itself in those who have unrepaired cleft or recent repair of cleft, and also the families with children who have cleft. 2) Repair. Clefts can be cured. So it’s making sure we can identify those kids with cleft, give them care, and support the development of high-quality surgical services to take care of these kids and cure them.” To maximize the reach of prevention, identification, nutritional support, and surgical treatment services among the under-5 global population with cleft and their families, efforts must also take into consideration the disruptions to health services caused by the COVID-19 pandemic, widespread food shortages, and the remaining unmet needs of families.
Read more in Think Global Health: The Cleft Palate-Malnutrition Connection