
Targeting the health of adolescents in India
Published November 21, 2016
Adolescence is often overlooked in health policy and planning, despite the fact that it represents a crucial period of life for addressing risks and preventing health problems in later life. Guided by insights from the Global Burden of Disease (GBD) study, the Government of India has prioritized the needs of adolescents in a comprehensive strategy to address the determinants of poor health for women, children, and young people.
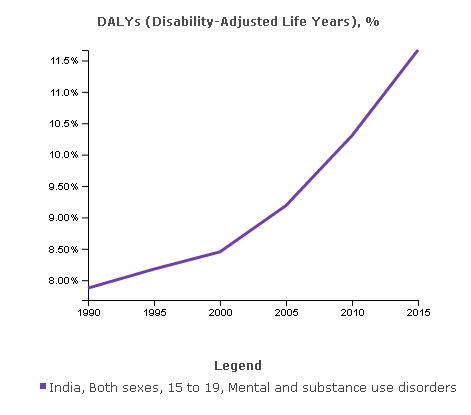
In India, as in the rest of the world, adolescents face a number of challenges to their health and well-being. The GBD study, led by the Institute for Health Metrics and Evaluation (IHME), shows that mental and substance abuse disorders are on the rise among Indian youth aged 15–19, accounting for 12% of the total DALYS for this age group in 2015. Moreover, 13% of all adolescent health loss in India is attributable to behavioral risk factors such unsafe sex, poor nutrition, smoking, and alcohol and drug use, and exposure to many of these risks also sets the stage for the onset of non-communicable diseases in adulthood.
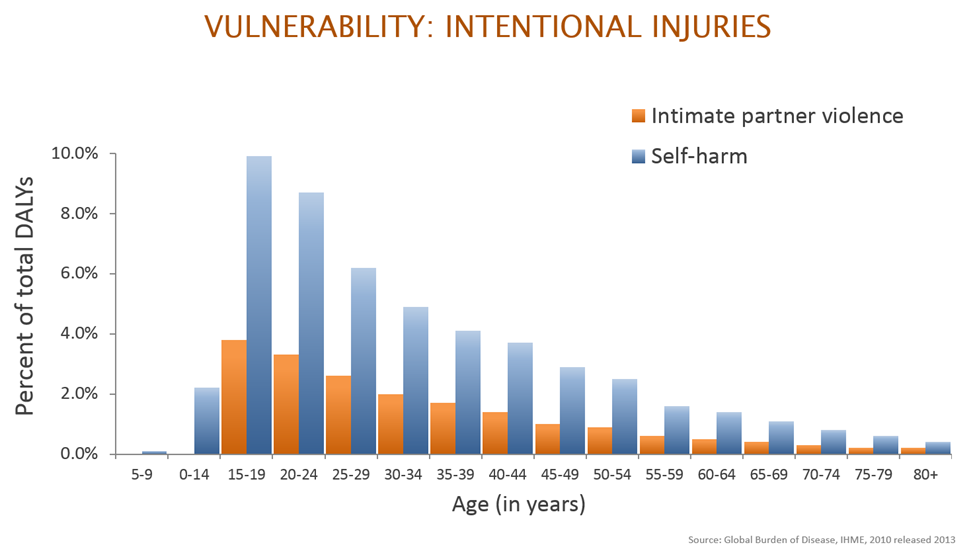
Injury is another serious problem for adolescents, accounting for over 20% of premature death and disability. Breaking this down further, GBD data reveal that adolescents are the age group most vulnerable to sexual abuse, as well as intentional injuries as a result of intimate partner violence and self-harm. This is demonstrated in the image below, one of many figures featuring GBD data used by Ms. Anuradha Gupta, Additional Secretary and Mission Director of the National Health Mission in the Ministry of Health and Family Welfare, to make a strong case for targeting adolescent health.
Informed by this evidence, India’s Ministry of Health & Family Welfare for the first time included adolescence as a distinct life stage in its latest maternal and child health strategy: the RMNCH+A (reproductive, maternal, newborn, child, and adolescent health). It lays out five priority interventions for this age group: nutrition and supplementation; adolescent-friendly health clinics for reproductive and sexual health; information and counseling on sexual health, mental health, and substance use; the promotion of menstrual hygiene; and preventive health check-ups for disease screening.
These interventions provide access to vital health services but they are also responsive to the fact that many adolescent health issues, particularly those of girls and young women, have deep social and cultural determinants. As such, education is at their heart. For instance, in order to address gender-based violence the Ministry aims to provide comprehensive life skills education that will “improve knowledge, attitudes, and behaviors regarding sexual and reproductive health [and] promote favorable attitudes against gender-based violence,” thus equipping young people with the “awareness and skills to challenge gender stereotypes, discrimination, and violence.”
What happens in adolescence has long-term repercussions for a person’s health throughout their life, and has significant intergenerational causes and effects. RMNCH+A sets out a comprehensive, holistic approach to health that acknowledges that improving outcomes cannot be done in isolation; rather, it requires a life cycle approach which ties together maternal, child, and adolescent health in a coordinated continuum of care. By linking each of these life stages with facility-based care and a set of cross-cutting interventions, along with continuing to strengthen health system capacity, the government seeks to achieve marked improvements in India’s health landscape. With GBD evidence supporting the necessity of a focus on adolescence, the Ministry of Health and Family Welfare has been able to fine-tune its approach to effectively address the country’s specific health needs, and make steps toward reducing the burden of disease and violence on India’s youth.